Opioids and Acute Pain Management
Opioids overdose has become a public health emergency. In 2018, of every three overdose deaths two were related to opioids. Of a total of 47, 000 deaths associated with opioids in 2018, 32 % of those deaths were related to prescribed opioids. Several studies have shown disproportionate prescriptions of opioids after ER visits and surgical procedures of which patients save leftover pills. Therefore it is important to responsibly prescribed opioids, while at the same time treating patients’ pain appropriately. Opioids are often reserved for patients with acute severe pain, postoperative, chronic malignant and non-malignant pain. When treating acute pain, opioids should be prescribed in the lowest dose and for a shorter period of time. So what are the recommendations when prescribing opioids home regimens for acute pain management?
Before diving into those recommendations, let’s talk about opioids a little bit more.
Mechanism of action Opioids can provide antidiarrheal, analgesic and antitussive relief. But as per analgesic effects, opioids work by inhibiting the neuron synaptic activity through opioid receptor activation and release of body endogenous opioid peptides which causes further neuron inhibition. When opioids receptors are activated at the postsynaptic side, it causes hyperpolarization of the neuron by opening k+ channels. Activation of opioids channels at the presynaptic levels prevent release of neurotransmitters such as acetylcholine, norepinephrine, serotonin, glutamate and substance p (related to pain).
The three major opioids receptors, mu, delta and kappa, are located afferent and spinal cord neurons responsible for pain transmission as well as for neurons in the midbrain and medulla responsible for pain modulation. Other opioid receptors located in neurons in the ganglia, hypothalamus, limbic structures and cerebral cortex are involved in reactivity to pain.
Opioids Classification
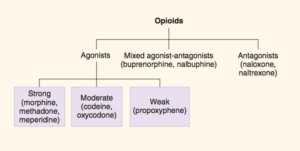
Opioids are classified as agonist, antagonist and mixed agonist-antagonist. Agonists are further classified as full or partial agonists based on their ability to activate the receptors. Based on their ability to provide pain relief, agonists are categorized as strong, moderate and weak. Mixed agonist-antagonist opioids have the ability to block or activate certain subtypes of receptors.
Management of Acute Pain
Now, what are the recommendations when sending patients home with opioids for the management of acute pain? When prescribing opioids, there are always the concerns for their misuse and abuse, especially in patients without a history of previous opioids treatment. Therefore, it is recommended to prescribe short-acting opioids instead of long-acting or extended release for acute pain in patients without previous record of opioids use. Short-acting opioids can provide relief in 45 to 60 minutes as opposed to extended-release which have a peak effect in 3 to 4 hours. There is a greater chance of unintentional overdose with long-acting opioids. It is also recommended to prescribe a 3 day supply for pain related to non-surgical procedures or not related to trauma. For pain after surgery or trauma, adequate opioid supply can be prescribed until a follow-up appointment.
Some commonly prescribed opioids include oxycodone, hydrocodone, codeine and tramadol, but codeine and tramadol are prescribed to a lesser degree. As per oxycodone and hydrocodone, UptoDate suggest a few acute pain regimen depending of pain severity:
Mild pain (caused by sprains, nonspecific low back pain, dental extraction, and headaches) → Opioids should not be prescribed. Non-opioid medication is preferred.
- Acetaminophen
- NSAIDs
- COX- 2 inhibitors
Moderate pain (caused by laparoscopic procedures, minimal invasive surgery, soft-tissue surgery, non-compound/comminuted fracture) → a 3 day supply of short-acting opioids can be prescribed.
- Oxycodone 5mg, 3-4 pills per day
- Hydrocodone 5mg, 3-4 pills per day
- Hydromorphone 2mg, 3-4 pills per day
Severe pain (major surgery, maxillofacial surgery, total joint replacement, compound/ long bone fractures) → higher dose for 7 days if follow- appointment is scheduled within 7 days.
- Oxycodone 5mg, 4-6 pills per day
- Hydrocodone 5mg, 4-6 pills per day
- Hydromorphone 2mg, 4-6 pills per day
If applicable, incorporate others non-pharmacological regimens such as ice, heat, elevation, immobilization, rest, relaxation etc. Establish with the patient that the goal of the treatment is not “zero pain,” but rather making the pain more tolerable. Decrease opioids dosage quickly, and advise patients to continue with the non-pharmacological and non-opioid regimens.
Adverse Effects of Opioids Aside from the dependency, addiction and overdose risks, adverse effects of opioids include:
- Nausea, vomiting, fatigue, dysuria (most common)
- Respiratory depression
- Sedation and confusion
- Depression
- Insomnia
- Opioid hyperalgesia
- Constipation
- Osteopenia
- Hypotension
- Immune system impairment
Always be vigilant for signs of opioid abuse and identify intoxication promptly as symptoms appear such as euphoria, drowsiness, constricted pupils, hypotension, bradycardia, hypothermia, coma and respiratory arrest. Treat with naloxone and supportive care.
Sources:
- https://accessmedicine-mhmedical-com.york.ezproxy.cuny.edu/ViewLarge.aspx?figid=217402515
- https://www-uptodate-com.york.ezproxy.cuny.edu/contents/prescription-of-opioids-for-acute-pain-in-opioid-naive-patients?search=pain%20emergency%20department%20management&source=search_result&selectedTitle=1~150&usage_type=default&display_rank=1#H1334178472
- https://www.cdc.gov/drugoverdose/data/index.html
- Smollin, Craig, and Kent R. Olson.. “Opiate & Opioid Overdose.” Current Medical Diagnosis and Treatment 2020 Eds. Maxine A. Papadakis, et al. New York, NY: McGraw-Hill, , http://accessmedicine.mhmedical.com.york.ezproxy.cuny.edu/content.aspx?bookid=2683§ionid=225059427.
- KatzungTrevorPharm11th Ed(2015).pdf